
1. Introduction
Noise research in hospitals focuses mainly on the harmful effects on patients [2; 5; 8]. But at least in intensive care units and operation rooms, also the staff is exposed to high levels of noise during considerable portions of working time. [1; 3; 4; 6 – 8]. In operating rooms sound levels as well as demands on the staff are quite high.
The noise exposure levels reported above from several international studies are not high enough to be considered as a danger for hearing. However, according to the present knowledge of the research on effects of noise, these high average levels and maximum levels – sometimes with a portion of high frequencies – are strong enough to elicit physiological stress responses as well as eliciting disorders regarding communication and performance [4; 10; 12]. Speech comprehensibility is reduced by maximum levels from 55 dB(A) upwards; with sound level increasing further, concentration is disturbed, background speech becomes very irritating [11 – 13], and the number of mistakes rises constantly [14].
1.1 Recommended limit values are not met
With regard to the highly responsible work in hospitals, lower protective exposure limits for these workingplaces should be strived for, e.g., as provided for in the German guideline VDI 2058 with Leq
55 dB(A) for medical tasks. Still more demanding are the protective goals of the WHO for treatment rooms with Leq day
30 dB(A) and for patients’ rooms Leq by day 35 dB(A) and by night 30 dB(A) with maximum levels up to 40 dB(A). At present, however, these values seem to be far away from reality in our hospitals. Similar results are reported by [10] in a literature review study 2012 (see also 4). The new workplace regulation „ASR A3.7 Noise“ has been in force in German occupational safety law since May 2018. There, the level of noise may not exceed 55 dB (A) for activities that require constant high concentration, such as „…medical examinations, treatments and operations…“. Further requirements are set for the reverberation time.
In the United States, this problem has received attention in the past decade in the ecological context of „green hospitals“ (e.g., [15]).
1.2 Commitment to risk management
The theme of „(clinical) risk management“ attracts more and more importance for modern clinics. The effectiveness of the tool of clinical risk management was proved in several studies [16; 17].
In this process, a multitude of relevant national and international regulations make great demands on the operating authorities of the clinics concerning the implementation of a risk management in order to maintain the compliance of the clinics and its executives.
1.3 Deficiencies in patient safety
Safety of patients is a theme which is increasingly noticed internationally since the American report „To err is human“ was published at the turn of millennium [18]. The author ascertains in his report for the Institute of Medicine (IOM) that between 2.9 and 3.7 % of all patients admitted to hospitals suffer an „adverse event“, i.e., an injury due to the treatment. The same year, McNeil et al. published a report for the Victorian Government Department of Human Services in Australia, called „Improving patient safety in Victorian hospitals“, according to which about 16.6 % of all stationary admittances to hospitals lead to an “adverse event”. About 50 % of these „adverse events“ were classified as avoidable. Similar results are reported from the British Department of Health in the report „An organization with a memory – Report of an expert group on learning from adverse events in the NHS“ in 2000 and also from [21].
1.4 Handovers as critical points
In the study „Survey on the introduction of clinical risk management in German hospitals“, Lauterberg [19] found main emphasis of the study participants on the following risk profiles for general hospitals: clearly leading are problems at organizational cutting points (46,5 %), then drug therapy (34,4%) and hospital infections / hygiene (32,2%). Similar results are reported from Doms [20] in a legal article.
1.5 Significance of noise on performance and susceptibility to faults is little studied
Unfortunately, the importance of extra-aural effects of noise on performance and error-proneness of the employees is mostly not taken into account, although reduction of concentration and increase of numbers of mistakes is well documented [14]. Also background noises, especially speech, is often perceived as disturbing and distracting [11 – 13].
Depending on the amount of noise exposure, an increase of the number of mistakes in the activities of the medical staff can be assumed. If patients suffer damages due to mistakes of the medical staff and the person has acted in a legally culpable manner, the patient is entitled to claims for compensation and damages [20].
The aim of the entire study is the evaluation of the acoustic situation in a typical large hospital in Germany, and its relation to self-rated well-being and performance of the staff. This contribution specifically examines the relationship between acoustic stress, performance and the frequency of the resulting errors.
The research project in 2016 on „Mental Health in the Working World – Scientific Assessment“ of the German Federal Institute for Occupational Safety and Health (BAuA) also revealed in the „Noise“ section that noise leads to errors: „…In clinics, for example, the influence of level-oriented features in the operating theatre on the frequency of (post-operative) complications or errors by the surgeons was investigated. Here a reduction is shown as a result of measures to reduce noise…“.
2. Method
Setting: In the operating rooms of the hospital at the Park Lünen of Hospital Westphalia. The clinic was founded in 1907 and has currently 228 employees, with 6 departments with 160 beds. Each year, 6.250 inpatient patients and around 12.000 ambulatory patients are provided.
2.1 Accoustic measurements
Continuous measurements for at least
3 x 24 hours in one week in two identical OTs (OT 1 and OT 2), an OT (OR 3) and in the transition between OT1 / OT2 and the patients sluice were performed over a period of three weeks in the summer of 2015 (measuring instruments from Brüel & Kjær 2238 mediator; calibrator: Brüel & Kjær 4231). OT 3 differs from the first two operating rooms and is located at the end of the corridor, separated by a smoke control door right next to the locker room. Firstly, it is smaller than the first two (the ceiling height is also low) and secondly, it is set up differently and the ENT surgeries are performed there (such as operations on the jaw bone, paranasal sinuses, removal of the pharyngeal tonsil etc.). In OT1 and OT2, operations from the fields of general surgery, trauma surgery and orthopaedics were performed. The measurements were usually set up on Sunday afternoons and removed at the end of the week. The reverberation as a defining room acoustic parameter was identified as well.
2.2 Measurement of staff:
At the same time the strain of the staff was measured with a set of standardized questionnaires. At the end of each of their shifts the employees were requested to fill out a „Questionnaire on the acoustic situation“ in which they should state, among others, how loud they perceived the shift and which noise-induced impairments or noise-induced errors they encountered.
2.3 Statistical Analysis:
All analyses were made with SPSS statistical package (version 24). We used generalized linear mixed models (GLMM). Due to the fact that different people answered a different number of questionnaires each referring to a different workday in the OT, we considered the subjects as a constant term.
3. Results
3.1 Sound level measurements
in the OTs
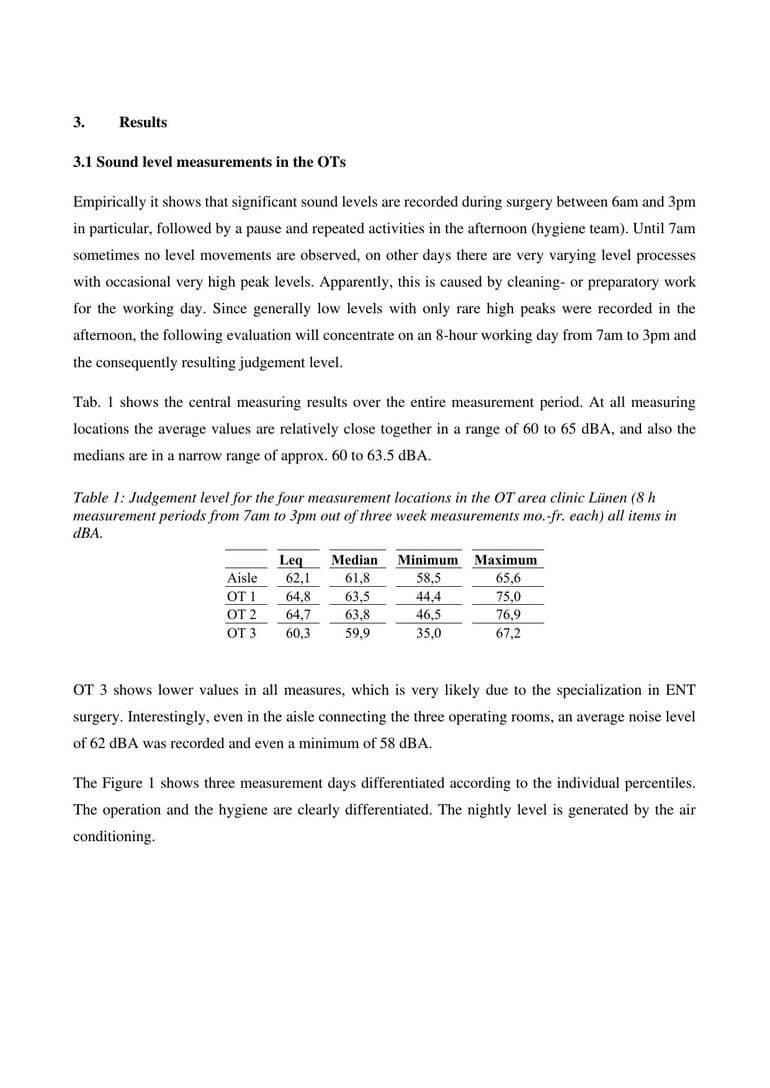
Empirically it shows that significant sound levels are recorded during surgery between 6am and 3pm in particular, followed by a pause and repeated activities in the afternoon (hygiene team). Until 7am sometimes no level movements are observed, on other days there are very varying level processes with occasional very high peak levels. Apparently, this is caused by cleaning- or preparatory work for the working day. Since generally low levels with only rare high peaks were recorded in the afternoon, the following evaluation will concentrate on an 8-hour working day from 7am to 3pm and the consequently resulting judgement level.
Tab. 1 shows the central measuring results over the entire measurement period. At all measuring locations the average values are relatively close together in a range of 60 to 65 dBA, and also the medians are in a narrow range of approx.
60 to 63.5 dBA.
OT 3 shows lower values in all measures, which is very likely due to the specialization in ENT surgery. Interestingly, even in the aisle connecting the three operating rooms, an average noise level of 62 dBA was recorded and even a minimum of 58 dBA.
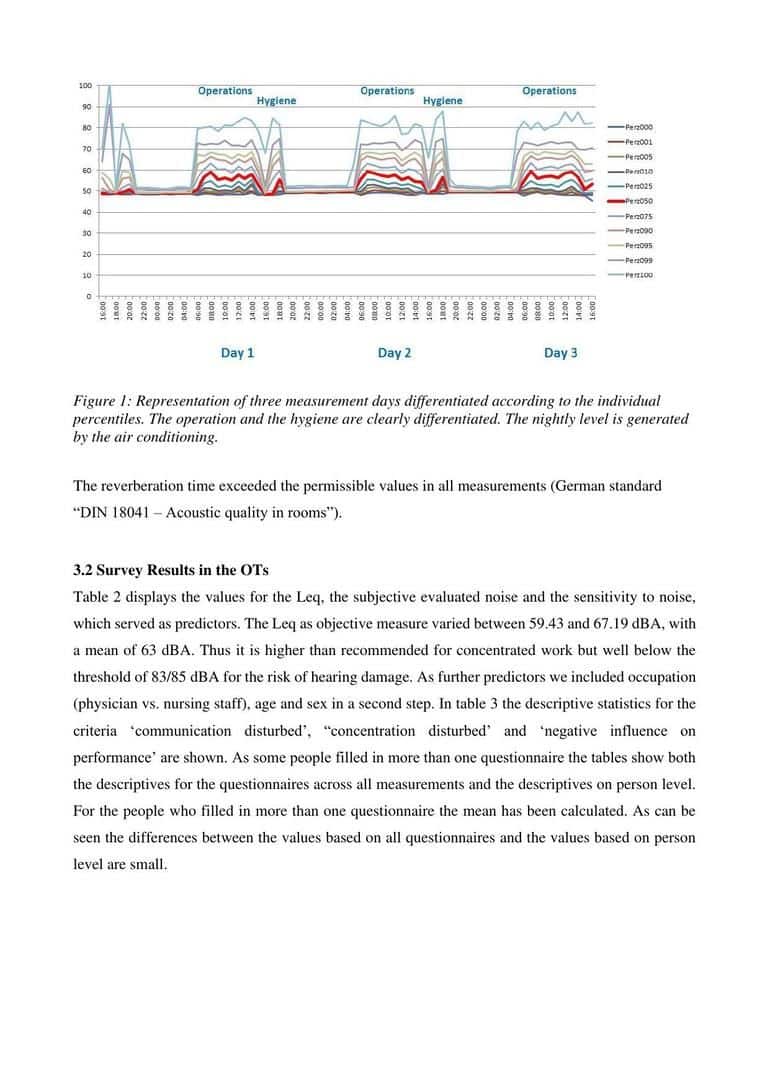
The Figure 1 shows three measurement days differentiated according to the individual percentiles. The operation and the hygiene are clearly differentiated. The nightly level is generated by the air conditioning.
The reverberation time exceeded the permissible values in all measurements (German standard “DIN 18041 – Acoustic quality in rooms”).
3.2 Survey Results in the OTs
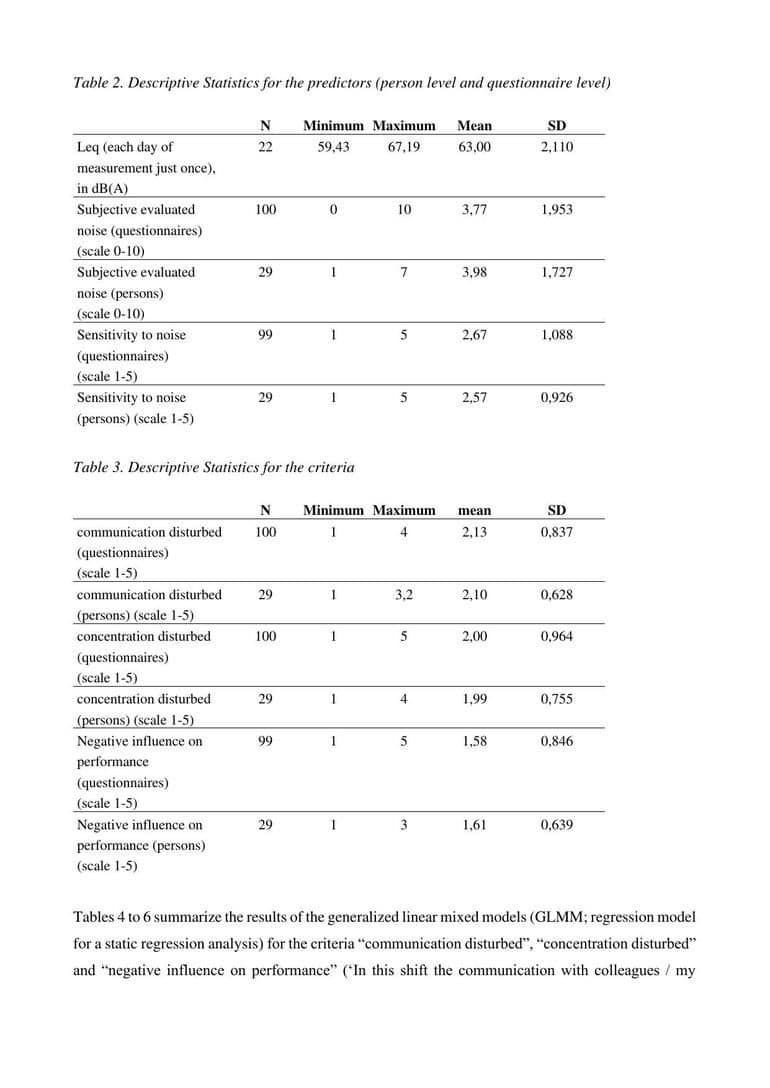
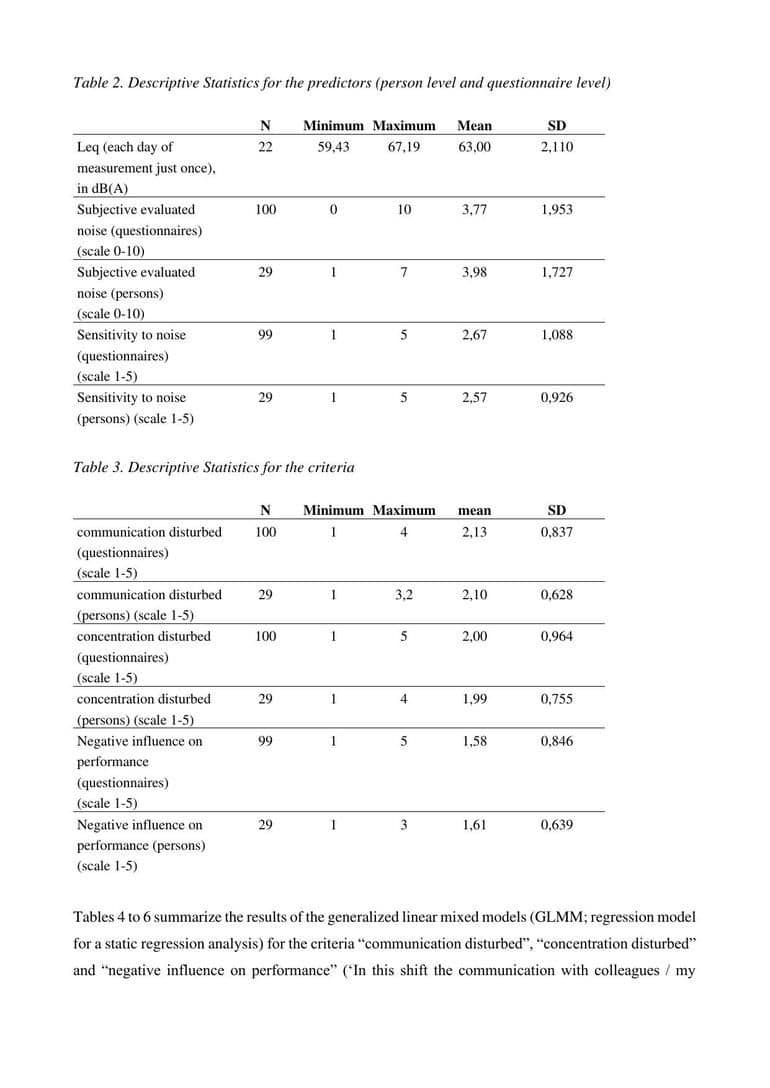
Table 2 displays the values for the Leq, the subjective evaluated noise and the sensitivity to noise, which served as predictors. The Leq as objective measure varied between 59.43 and 67.19 dBA, with a mean of 63 dBA. Thus it is higher than recommended for concentrated work but well below the threshold of 83/85 dBA for the risk of hearing damage. As further predictors we included occupation (physician vs. nursing staff), age and sex in a second step. In table 3 the descriptive statistics for the criteria ‘communication disturbed’, “concentration disturbed’ and ‘negative influence on performance’ are shown. As some people filled in more than one questionnaire the tables show both the descriptives for the questionnaires across all measurements and the descriptives on person level. For the people who filled in more than one questionnaire the mean has been calculated. As can be seen the differences between the values based on all questionnaires and the values based on person level are small.
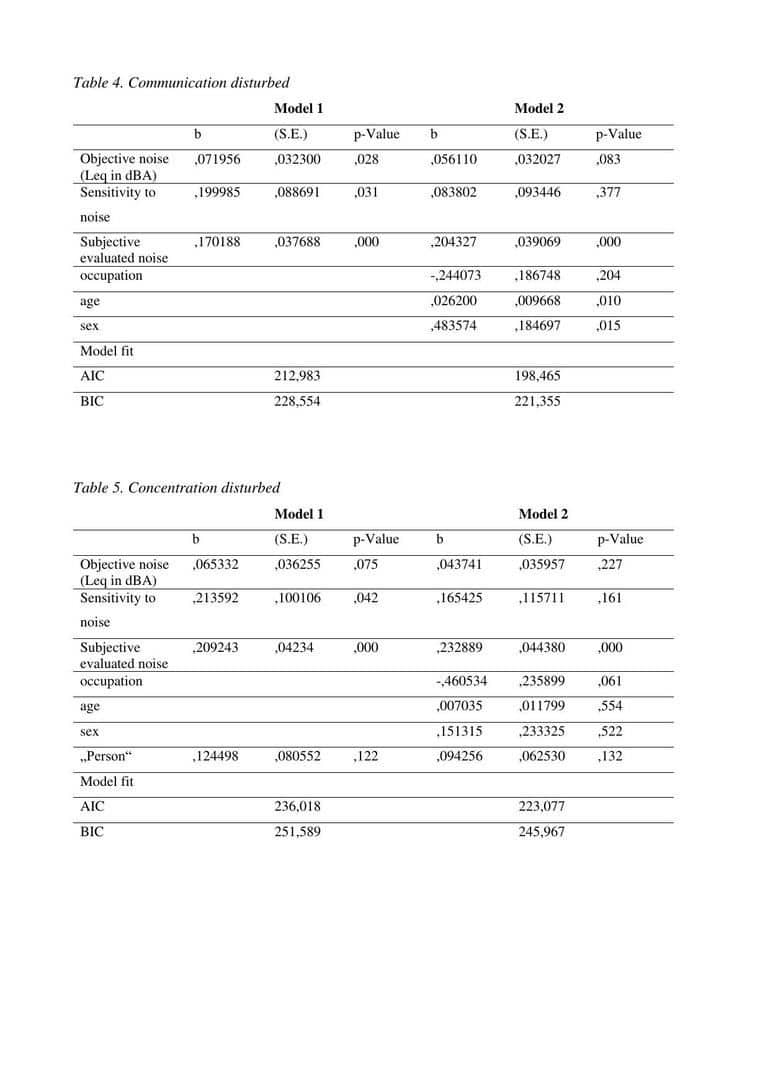
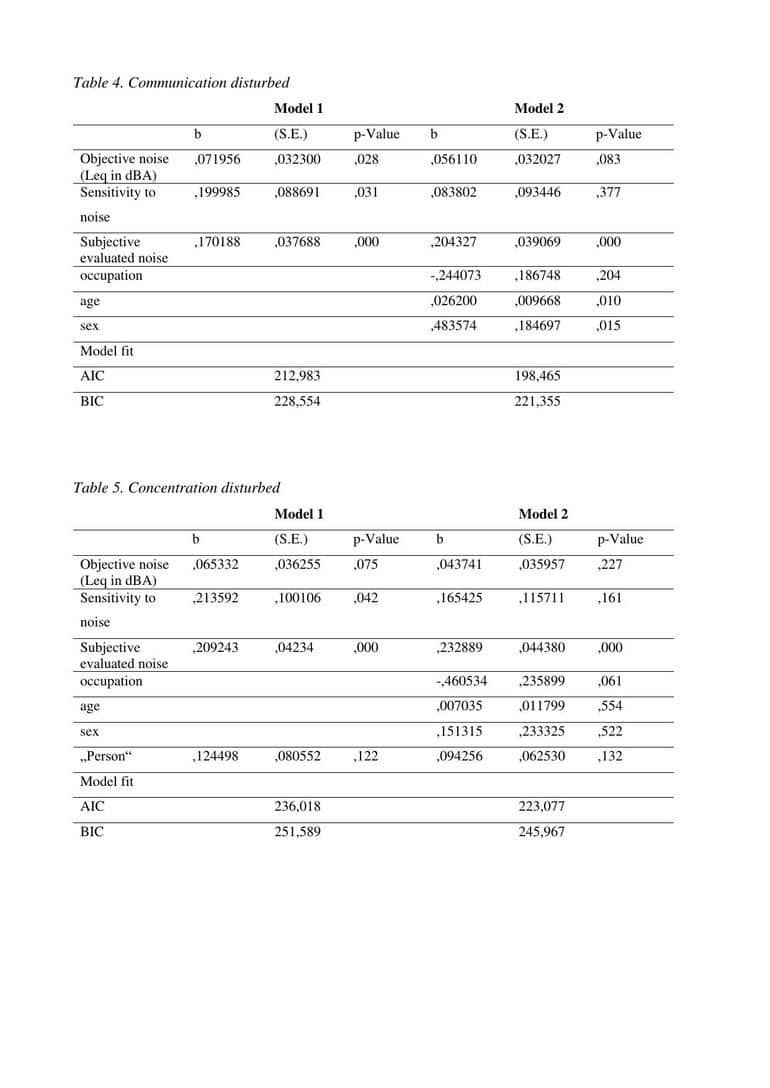
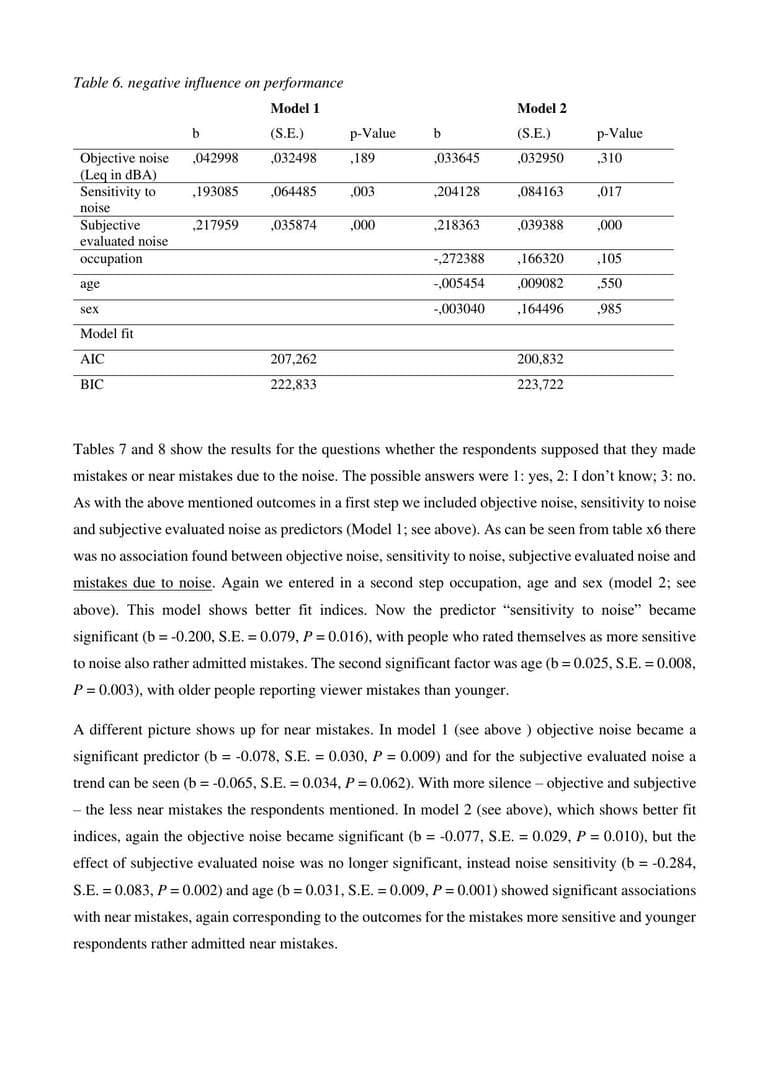
Tables 4 to 6 summarize the results of the generalized linear mixed models (GLMM; regression model for a static regression analysis) for the criteria “communication disturbed”, “concentration disturbed” and “negative influence on performance” (‘In this shift the communication with colleagues / my concentration was disturbed by noise or sound’, ‘In this shift my work performance was negatively influenced by noise or sound’: scale: 1 (not at all) to 5 (extremely)).
Model 1: First we entered the factors “objective measured noise” (noise measured in dBA), “subjective evaluated noise” (‘On the whole, how loud was it today during your work?’, 0–10), sensitivity to noise (‘are you sensitive to noise?’, 1–5). The objective measured noise just became significant for the factor ‘communication disturbed’. (b = 0.072, S.E. = 0.032, P = 0.028), indicating the increase in disturbed communication by the factor 0.072 for every decibel, as seen in table 4. The sensitivity to noise served as significant predictor for each of the criteria ‘communication disturbed’ (b = 0.200, S.E. = 0.089, P = 0.031), ‘concentration disturbed’ (b = 0.214, S.E. = 0.100, P = 0.042) and ‘negative influence on performance’ (b = 0.193, S.E. = 0.064, P = 0.003). Thus indicating an increase by the factor 0.200 in the scale “disturbed communication”, 0.214 in the scale “disturbed concentration” and 0.193 in the scale “negative influence on performance” for each point more in sensitivity to noise. And also the factor “subjective evaluated noise” served as significant predictor for all three criteria (‘communication disturbed’: b = 0.170, S.E. = 0.038, P = 0.000; ‘concentration disturbed’: b = 0.209, S.E. = 0.423, P = 0.000; and ‘negative influence on performance’: b = 0.218, S.E. = 0.036, P = 0.000). Thus both the trait-factor “sensitivity to noise” and the state-factor “subjective evaluated noise” are associated with all three measured outcomes, whereas the objective measured noise is just associated with disturbed communication.
Model 2: In a second step we entered the factors occupation (1: physician vs. 2: nursing staff), age and sex (1: male, 2: female). As can be seen from the tables 4 to 6 except for BIC at “negative influence on performance” the fit indices AIC and BIC (information criteria in GLMM) got better by introducing these three factors. Occupation was not significantly associated with “communication disturbed” and “negative influence on performance” and was just marginal significantly associated with “concentration disturbed” (P = 0.061), with the physicians tending to be more disturbed than the nursing staff. Age and sex were just associated with “communication disturbed (age: b = 0.026, S.E. = 0.010, P = 0.010; sex: b = 0.484, S.E. = 0.185, P = 0.015) indicating that older and female persons tended to perceive more disturbance of communication. Also interesting is that “sensitivity to noise” lost its effect on the outcomes “communication disturbed” and “concentration disturbed”.
The factor person did not reach significance for any of the outcomes in any of the models.
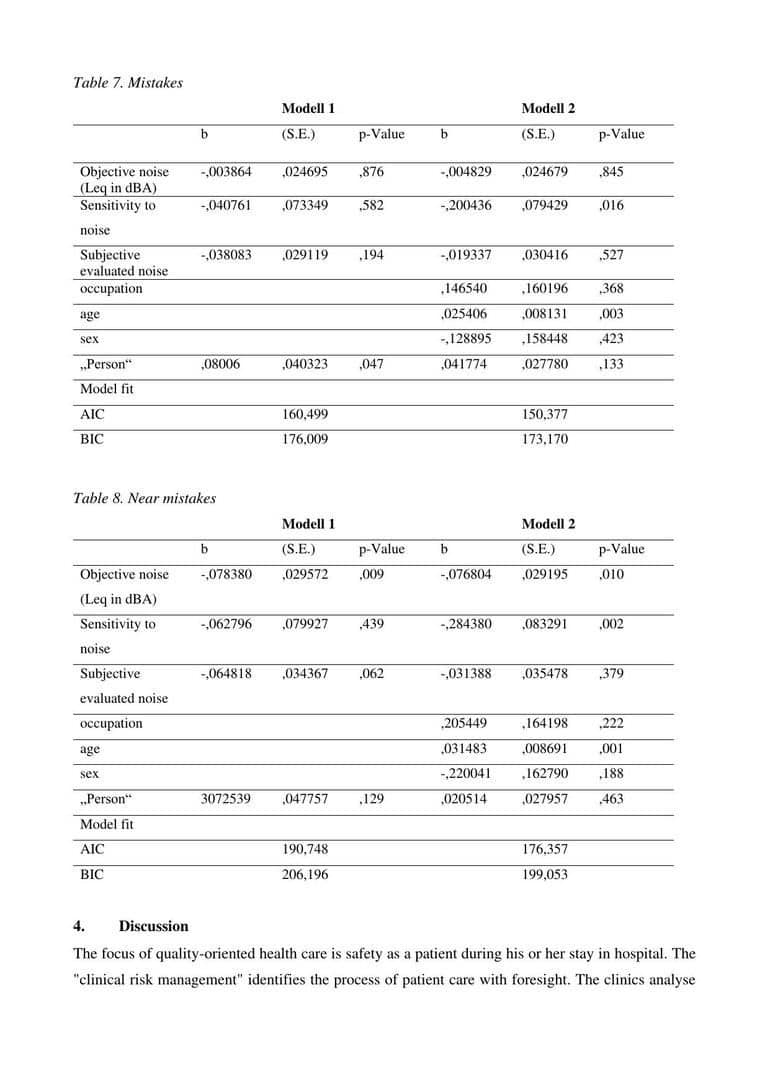
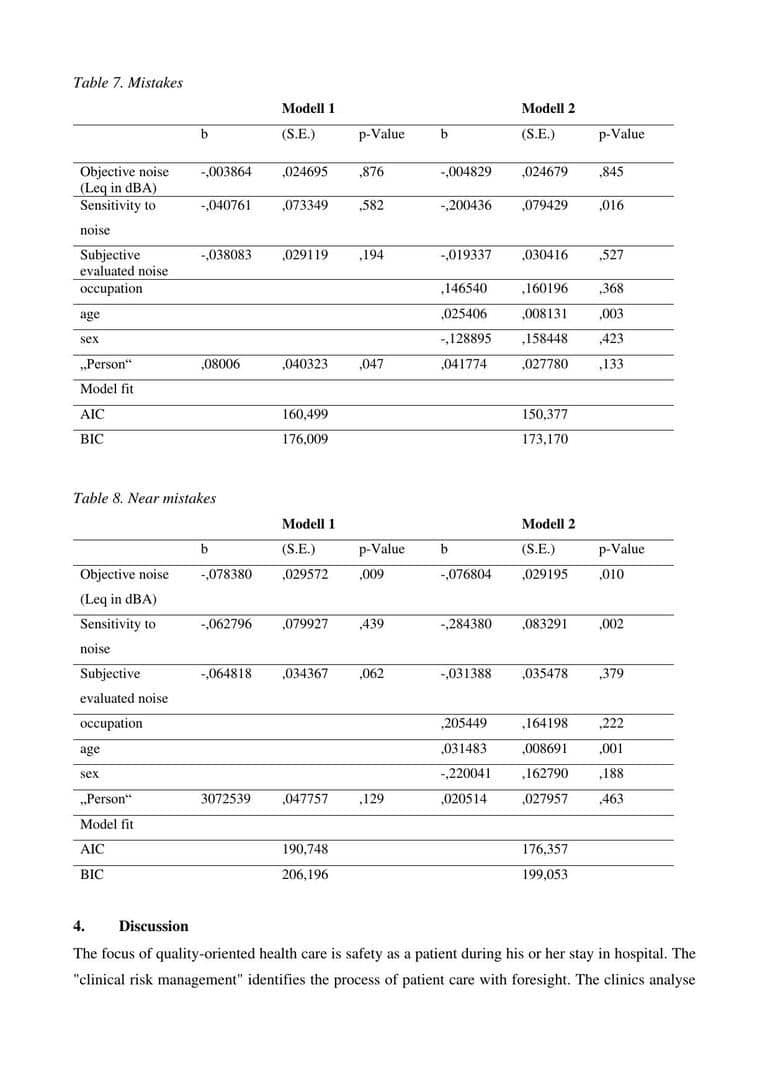
Tables 7 and 8 show the results for the questions whether the respondents supposed that they made mistakes or near mistakes due to the noise. The possible answers were 1: yes, 2: I don’t know; 3: no. As with the above mentioned outcomes in a first step we included objective noise, sensitivity to noise and subjective evaluated noise as predictors (Model 1; see above). As can be seen from table x6 there was no association found between objective noise, sensitivity to noise, subjective evaluated noise and mistakes due to noise. Again we entered in a second step occupation, age and sex (model 2; see above). This model shows better fit indices. Now the predictor “sensitivity to noise” became significant (b = –0.200, S.E. = 0.079, P = 0.016), with people who rated themselves as more sensitive to noise also rather admitted mistakes. The second significant factor was age (b = 0.025, S.E. = 0.008, P = 0.003), with older people reporting viewer mistakes than younger.
A different picture shows up for near mistakes. In model 1 (see above ) objective noise became a significant predictor (b = –0.078, S.E. = 0.030, P = 0.009) and for the subjective evaluated noise a trend can be seen (b = –0.065, S.E. = 0.034, P = 0.062). With more silence – objective and subjective – the less near mistakes the respondents mentioned. In model 2 (see above), which shows better fit indices, again the objective noise became significant (b = –0.077, S.E. = 0.029, P = 0.010), but the effect of subjective evaluated noise was no longer significant, instead noise sensitivity (b = –0.284, S.E. = 0.083, P = 0.002) and age (b = 0.031, S.E. = 0.009, P = 0.001) showed significant associations with near mistakes, again corresponding to the outcomes for the mistakes more sensitive and younger respondents rather admitted near mistakes.
4. Discussion
The focus of quality-oriented health care is safety as a patient during his or her stay in hospital. The „clinical risk management“ identifies the process of patient care with foresight. The clinics analyse and evaluate the risks and develop preventive measures. As part of risk management, they examine the structures and processes in the respective area of work in order to identify potential risks in a targeted manner. A comprehensive and sustainable clinical risk management system demonstrably leads to greater safety for patients and employees. Far too little attention is still paid to the risk factor „noise“.
5. References
G. Notbohm, S. Siegmann: Noise stress for patients in hospitals – a literature survey. Collected Papers, 21st. International Congress on Acoustics ICA, Montréal, Canada, J. Acoust. Soc. Am. 05/2013; 133(5):3553 (2013)
I. J. Bush-Vishniac: Noise levels in John Hopkins Hospital. J. Acoust. Soc. Am. 118, 3629–3645 (2005)
S. Siegmann, G. Notbohm: Noise in hospitals as a strain for the medical staff. Collected Papers, 21st. International Congress on Acoustics ICA, Montréal, Canada, J. Acoust. Soc. Am. 05/2013; 133(5):3453 (2013)
G. Notbohm, S. Siegmann: Workplace hospital: noise as a strain for the medical staff. Collected papers, Conference on Acoustics AIA-DAGA, Meran, Italy (2013)
S. Siegmann, G. Notbohm: Noise and sleep in hospitals – a review of literature. Collected papers, Conference on Acoustics AIA-DAGA, Meran, Italy (2013)
J. M. Kracht, I.J. Busch-Vishniac, J.E. West: Noise in the operating rooms of John Hopkins Hospital. J. Acoust. Soc. Am. 121, 2673–2680 (2007)
C. R. Engelmann, J. P. Neis, C. Kirschbaum, G. Grote, B. M. Ure: A noise-reduction program in a pediatric operation theatre is associated with surgeon‘s benefits and a reduced rate of complications: a prospective controlled clinical trial. Ann Surg., 259 (5), 1025–1033 (2014)
S. Siegmann, G. Notbohm, R. Schmook, N. Anduleit, K. Schöne, H. Sauer, P. Angerer: Noise pollution in a german hospital: Level measurement and survey results on the wards. Collected papers, 46th International Congress and Exposition on Noise Control Engineering INTERNOISE, Hong Kong, China (2017)
G. Notbohm, S. Siegmann: Lärmbelastung von Personal und Patienten im Krankenhaus – eine aktuelle Literaturauswertung, In: Jahrestagung für Akustik DAGA 2012 der Deutschen Gesellschaft für Akustik (DEGA), Darmstadt, 2012
G. Notbohm, S. Siegmann, P. Angerer: „Arbeitsplatz Krankenhaus: Lärmbelastung und Ansätze zur Prävention, Dokumentation der 52. Jahrestagung der Deutschen Gesellschaft für Arbeitsmedizin und Umweltmedizin (DGAUM), Göttingen, 2012
S. J. Schlittmeier, A. Liebl: Akustik im Büro: Zur Störwirkung von Hintergrundsprache (Office acoustics: The interference of background language). Lärmbekämpfung 6, 183–189 (2012)
S. B. Banbury, D. C.: Office noise and employee concentration: Identifying causes of disruption and potential improvements. Ergonomics 48, 1, 25–37 (2005)
E. Sundstrom, J. P. Town, R. W. Rice, D. P. Osborn: Office noise, satisfaction and performance. Environ. Behav. 26, 2, 195–222 (1994)
H. Ising, C. Sust, P. Plath: Lärmwirkungen – Gehör, Gesundheit, Leistung, Schriftenreihe Gesundheitsschutz, 4, Dortmund, Germany, (2004)
R. Ulrich, X. Quan, C. Zimring, A. Joseph, R. Choudhary: The Role of the Physical Environment in the Hospital of the 21st Century: A Once-in-a-Lifetime Opportunity. The Center for Health Design, online Publication (https://www.healthdesign.org/system/files/Ulrich_Role% 20of%20Physical_2004.pdf, 24.06.2020) (2004)
A. B. Haynes, T.G. Weiser, W. R. Berry et al.:
A surgical safety checklist to reduce morbidity and mortality in a global population. The New England journal of medicine 360 (5), 491–499 (2009)
M. E. Semel, S. Resch, A. B. Haynes, L. M. Funk, A. Bader, W. R. Berry, T. G. Weiser, A. A. Gawande: Adopting a surgical safety checklist could save money and improve the quality of care in U.S. hospitals. Health Aff, 29 (9), 1593–1599 (2010)
L. T. Kohn, J. M. Corrigan, M. S. Donaldson (ed.): To err is human: Building a safer health system, National Academies Press, Washington DC, USA (2000)
J. Lauterberg: Befragung zum Einführungsstand von klinischem Risiko-Management (kRM) in deutschen Krankenhäusern, Institut für Patientensicherheit der Universität Bonn (IfPS), Germany (2012)
T. Doms: Transparenz als beste Vorsorge, Dtsch. Arztebl. 102:A, 3, 117–118 (2005)
C. Vincent, G. Neale, M. Woloshynowych: Adverse events in British hospitals:preliminary retrospective record review. BMJ. 3; 322 (7285): 517–519 (2001)


